 Corner Bower & Rookwood Avenues
Corner Bower & Rookwood Avenues

Use this form to outline your medical history to us. We use this information to make informed dental care decisions about you.
The form is submitted securely and your information is stored confidentially. Your information is only shared to other medical professionals if you give permission.
Before starting
You will need this information handy before completing the form:
- your usual doctor's name and contact details
- records or memory of any medical procedures you have had, diseases you have, allergies etc etc.
If you prefer to print out a form, download the PDF in the panel below. Then you can post, fax, or bring the completed form to our office.
Form download
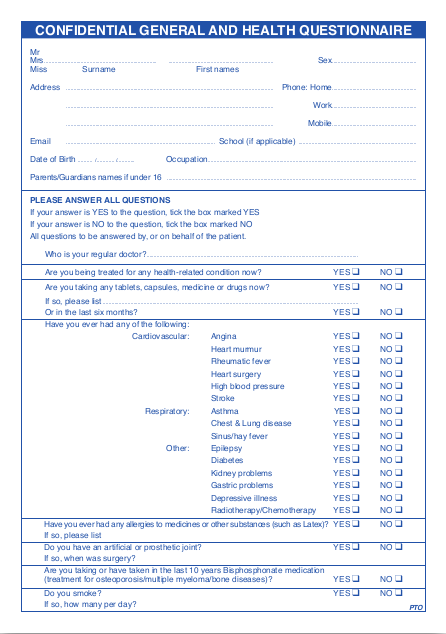
Confidential General and Health Questionnaire
Print this form out, fill it in, and bring it in for us if you prefer.